Case Report
Aggressive NK/T-Cell Leukemia With Aberrant CD20 Expression: A Case Report and Literature Review
Luther Fleury,1, Dapeng Wang,2, Naimy Rodriguez,3, Ling Zhang,2, Lugen Chen4*
1Department of Pathology and Cell Biology, University of South Florida Morsani College of Medicine, Tampa, FL; 2Department of Pathology, H Lee Moffitt Cancer Center, Tampa, FL; 3Department of Internal Medicine, Hospital Universitario Dr. Roman Ruiz Arnau, Bayamon, PR; 4Department of Pathology, Tampa General Hospital, Tampa, FL.
Abstract
Immunophenotypic aberrancy is not uncommon in B-cell hematologic malignancies. However, this phenomenon has infrequently been reported in NK/T cell neoplasms and is considered rare among aggressive NK/T cell leukemia. We report the case of a 53-year-old female who presented with 3 weeks of epigastric pain; leukocytosis, anemia, and thrombocytopenia; and markedly elevated transaminase and lactic acid. Serum Epstein-Barr virus (EBV) polymerase chain reaction (PCR) quantification peaked at 32x106 copies/mL. Imaging revealed significant hepatomegaly but no lymphadenopathy. A liver biopsy showed sinusoidal-to-focal diffuse infiltrate of atypical lymphoid cells with CD3+, CD5-, and CD20+ immunophenotypes identified via immunohistochemistry. This caused a diagnostic dilemma. Concurrent flow cytometry performed on the patient’s peripheral blood confirmed that these cells had the NK-cell phenotype (surface CD3-, cytoplasmic CD3+, CD2+, CD7+, CD56+, TCRαβ-, and TCRrδ-). The subsequent bone marrow biopsy demonstrated patchy involvement by the EBV+ neoplastic NK cells associated with prominent hemophagocytosis, supporting a diagnosis of aggressive NK-cell leukemia (ANKL). PCR further confirmed no evidence of T- or B-cell gene rearrangements. To the best of our knowledge, ANKL with aberrant CD20 expression has not been well described and could be a significant diagnostic pitfall. Because of its aggressive nature and frequent association with lethal hemophagocytic syndrome, it warrants immediate investigation to clarify the etiology of the aberrant CD20 expression as well as its significance regarding therapeutic decision-making.
Keywords
Aberrant expression, aggressive NK-cell leukemia, CD20, Epstein-Barr virus, NK/T-cell neoplasm
*Correspondence:
Lugen Chen, Department of Pathology, Tampa General Hospital, Tempa, FL 33606, USA. E-mail address: c-lchen@tgh.org
Introduction
Immunophenotypic aberrancy is not uncommon in hematologic malignancies. More frequently, hematopathologists come across T-cell marker aberrancies (e.g., CD5 aberrant expression) in small B-cell lymphomas, commonly chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and mantle cell lymphoma (MCL). Similarly, aberrant expression of B-cell markers, frequently CD20, has been seen in NK/T-cell neoplasms, but less commonly. In the literature, there are reports of CD20+ NK/T-cell neoplasms (e.g., extranodal NK/T-cell lymphoma, nodal NK/T-cell lymphoma, T-cell large granular lymphocytic leukemia, and T-cell prolymphocytic leukemia) [1-7] (Table 1); however, there is no report of aberrant expression of CD20 in aggressive NK-cell leukemia (ANKL).
ANKL is an aggressive lymphoproliferative disorder that is typically associated with an Epstein-Barr virus (EBV) infection (about 90% of cases) and is characterized by a fulminant clinical course [9, 10]. The immunophenotype for ANKL is surface CD3-, CD3 epsilon+, CD4-, CD5-, CD7+, CD16+ (variable), CD56+, and CD57- [8-10]. Aberrancies in ANKL have been reported in several large studies, but these aberrancies are typically marker losses (e.g., loss of CD2, CD7, or CD45); no studies have reported a gain of any B-cell marker [9]. We report, to the best of our knowledge, an ANKL with aberrant CD20 expression, a very unusual clinical scenario that has not been reported.
Case Report
A 53-year-old female with a past medical history of liver hemangiomas (patient had received radiation therapy 10 years prior) and fatty liver disease presented to an outside hospital and reported peripheral edema and worsening epigastric pain for 3 weeks. Initial CT imaging revealed hepatosplenomegaly but was otherwise unremarkable. The patient was febrile, dyspneic, and hypotensive, with laboratory results indicating leukocytosis (white blood cells [WBC] = 13.14×109/L), anemia (hemoglobin [Hgb] = 11.6 g/dL), thrombocytopenia (platelets = 82x109/L), elevated liver function tests (aspartate aminotransferase [AST] = 406 U/L, alanine aminotransferase [ALT] = 64 U/L, alkaline phosphatase [ALP] = 421 U/L), elevated creatinine (3.0 mg/dL), and rising lactic acid (10 mmol/L). Viral studies revealed a positive EBV IgG (749 U/mL). A liver biopsy was performed at the local hospital.
Given the patient’s poor condition, she was transferred to our hospital for a possible liver transplant. The liver biopsy results received from the outside hospital revealed that the sinusoids of the liver were markedly expanded by atypical lymphocytes, which were phenotypically CD3+, CD5-, CD56+, and CD20+ and had a Ki-67 positivity greater than 70% by immunohistochemistry (IHC). This suggested a diagnosis for NK/T-cell malignancy. Upon admission, PCR quantification for EBV was performed; serum EBV copies were elevated, with a peak of 32 x 106/mL.
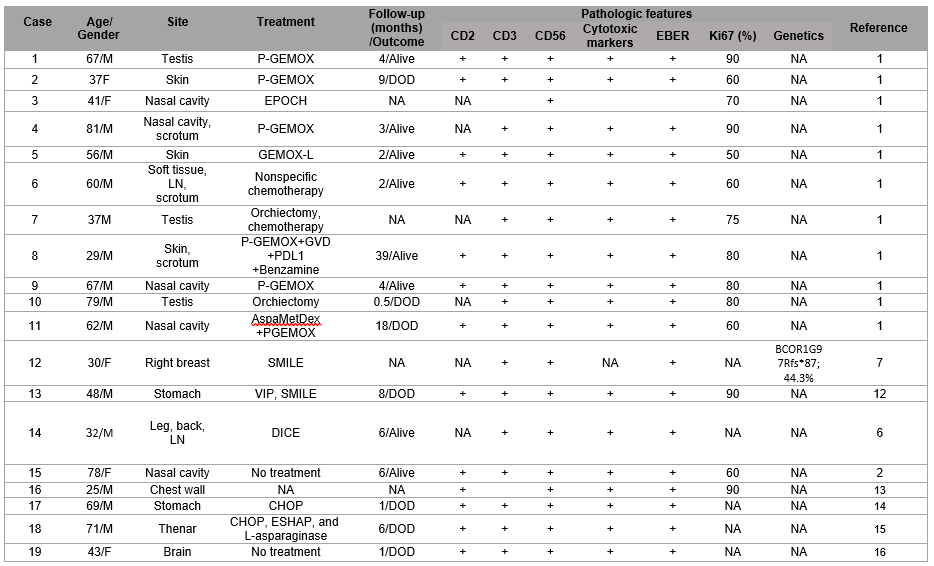
Table 1: Clinicopathologic features of CD20+ extranodal T/NK-cell neoplasms
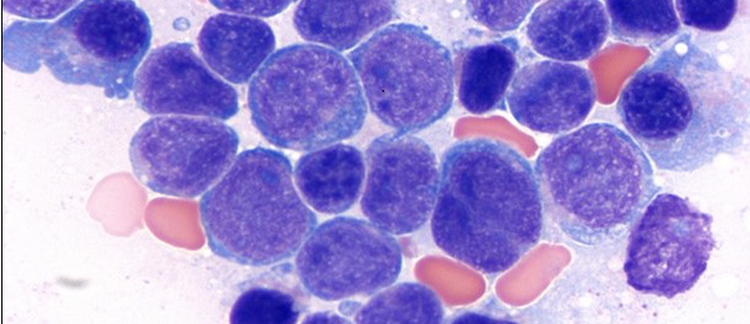
The peripheral blood smear revealed leukocytosis with many circulating large lymphoid cells with prominent nucleoli, irregular nuclear contours, and moderate cytoplasm containing large reddish granules. We identified circulating immature granulocytes but no myeloblasts, indicating left-shifted granulocytosis. Flow cytometry performed on the patient’s peripheral blood revealed an abnormal NK-cell population (18% of total events) that was positive for CD2, CD7, dim CD8, and CD56, with aberrant expression of CD20.
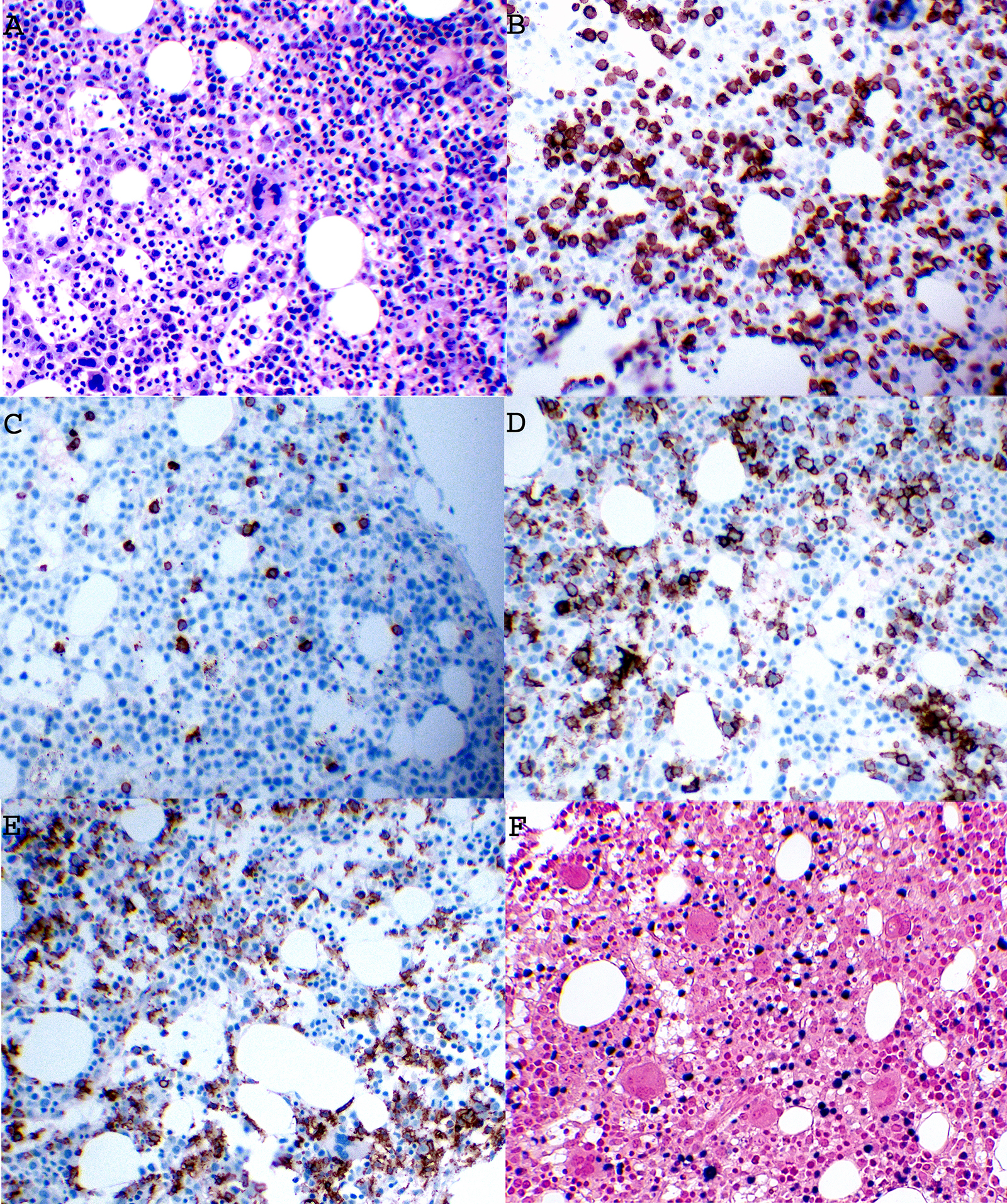
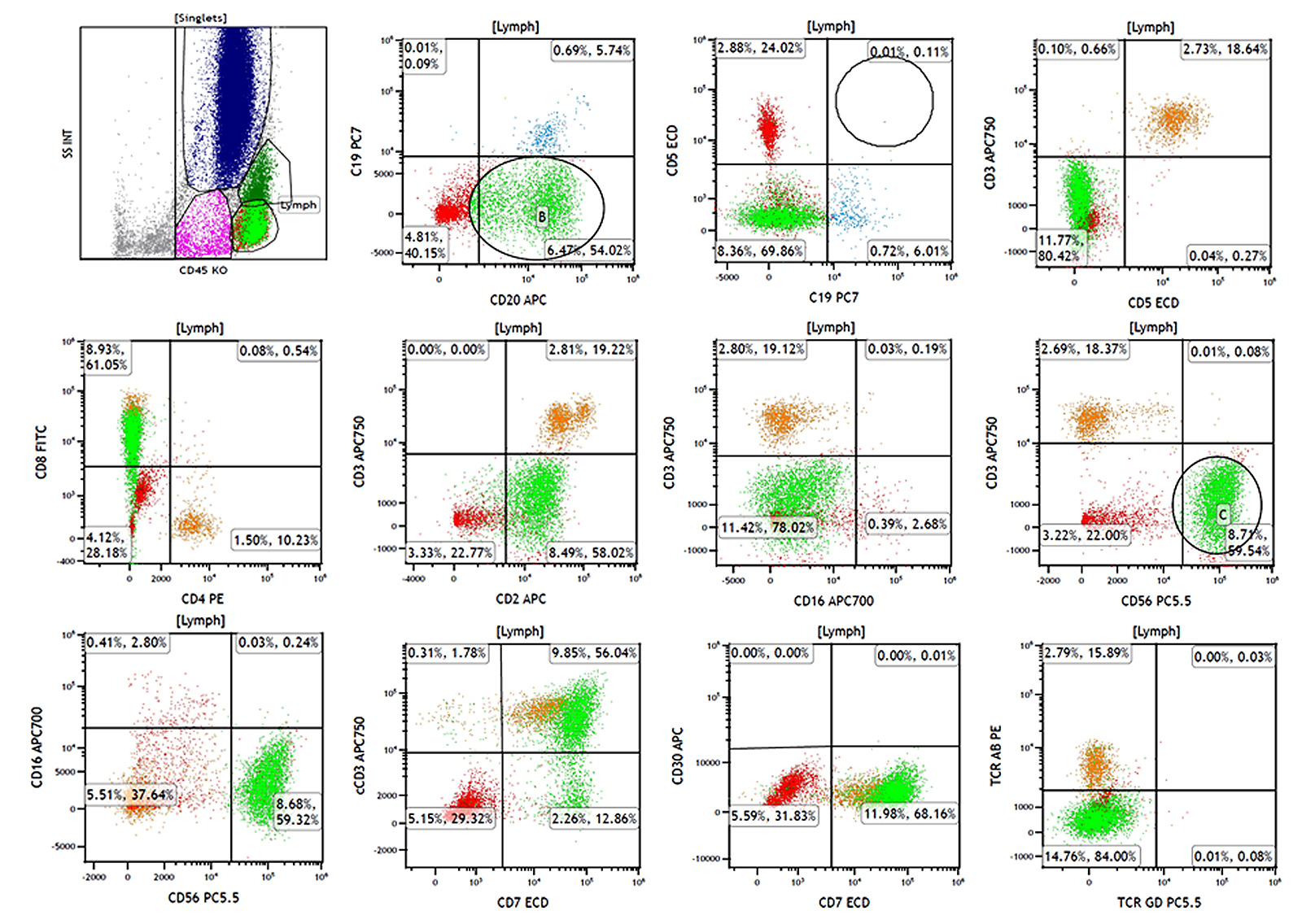
The bone marrow biopsy revealed hypercellularity (70%) with diffuse infiltration of abnormal NK cells and histiocytes with mild phagocytic activity (hemophagocytosis) (Figure 1). IHC performed on the biopsy revealed 30-40% of CD3+/CD20+ large lymphoid cells that were also positive for CD56, granzyme B, TIA-1, and EBV, as per in situ hybridization (ISH) with an EBV RNA probe. The neoplastic population was negative for CD5, PAX5, CD30, and CD57 (Figure 1). Flow cytometry performed on a bone marrow aspirate revealed an abnormal NK-cell population that was positive for CD2, CD7, dim CD8, CD56, and cytoplasmic CD3, with aberrant expression of CD20 (Figure 2). The population was negative for both TCR αβ and TCR rδ. In addition, PCR for B- and T- cell gene rearrangements performed on the original liver biopsy and peripheral blood samples were negative. All findings confirmed presence of an EBV-associated NK-cell population in peripheral blood, liver, and bone marrow with aberrant expression of CD20, supporting a diagnosis of ANKL.
During hospitalization, the patient’s condition continued to decline (renal failure, respiratory failure, and shock) despite treatment initiation (steroid, oxaliplatin, and gemcitabine). Though rituximab administration was considered and discussed with the patient’s family, it was not pursued due to the patient's deteriorated condition. The patient died approximately 10 days after the diagnosis of ANKL, which was approximately 6 weeks after reported symptom onset.
Discussion
CD20 is a transmembrane protein that has conventionally been thought of as a marker of B-cell lineage. Owing to the consensus that this marker is specific to B cells, CD20 is often used to confirm a suspicion of a B-cell neoplasm and differentiate between B-cell and T-cell neoplasms. Although aberrant B-cell marker expression by T-cell and NK-cell neoplasms is also a recognized phenomenon, it is quite rare [1, 2, 4, 6, 7]. In the available literature, NK-cell neoplasms with aberrant CD20 expression are even rarer than CD20-positive T-cell neoplasms [1, 2] due to the lower overall incidence of NK-cell neoplasms [11]. CD20-positive NK-cell neoplasms have been previously reported; however, all of them were found in extranodal NK/T-cell lymphomas [1, 2, 4, 7], and this phenomenon has not been well documented in ANKL, as was seen in our case. Table 1 includes the previously reported CD20+ extranodal NK/T-cell neoplasms in the English literature.
In general, patients with CD20+ extranodal NK/T-cell neoplasms (listed in Table 1; median age, 56 years; male to female ratio, 2.9) experienced similar aggressive clinical courses, with a median survival of 6 months. The most involved site was the nasal cavity, followed by the skin and testes. More than 80% (84%) of patients received chemotherapy, and none of them underwent allogeneic hematopoietic stem cell transplant. So far, there have been no diagnosed cases of CD20+ ANKL, as was seen in our current case, reported in the literature. This could be related to the rarity of ANKL, and the co-expression of CD20 could have been ignored or misinterpreted in other cases.
Understandably, due to the rareness of these NK/T-cell neoplasms (especially ANKL) and the aberrant expression of a well-recognized B-cell marker, reaching an accurate diagnosis was challenging [1, 10, 11]. Pathologists who encounter similar situations are encouraged to reference the patient’s clinical history and disease course in conjunction with their EBV status, an appropriate flow cytometry panel, IHC, and ISH to help ensure appropriate classification [11, 17]. Being aware of the existence of these rare aberrant findings is also helpful and can help prevent misdiagnosis when confronted with an overlap of various clinical, immunophenotypic, and morphologic features [1, 17]. Recommended IHC stains would include B-cell markers (CD20 and PAX5 or CD19 and CD79a), NK/T-cell markers (CD2, CD3, CD4, CD5, CD7, CD8, CD56, and TIA-1), and Epstein-Barr virus encoding region (EBER) ISH when an EBV-associated NK/T-cell neoplasm is suspected [1].
There are two main theories that may explain CD20 expression in NK/T-cell neoplasms. The first theory is that there is actually a very small population of NK/T cells that express CD20, or at least variably express it [1-4, 6]. There have been reports of small subsets of normal T lymphocytes in the blood that express CD20 at a low level, which gradually increases with age; in some cases, these are referred to as CD20dim T cells [2, 5]. In these cases, the neoplasm would be a lymphoproliferative disorder arising from a subset of normally benign CD20-positive T cells. The second theory is that the aberrant expression of CD20 is simply a manifestation of the neoplastic process [1-4, 6]. Tsai et al. [6] cited a case from a French cutaneous lymphoma group that presented a patient with mycosis fungoides with large-cell transformation with CD20 positivity that was not present at the initial diagnostic biopsy. Other potential mechanisms proposed in the literature include gene amplification and alterations in epigenetic regulation [1].
Naturally, the successful use of anti-CD20 therapeutics (e.g., rituximab, ibritumomab, and ocrelizumab) has led researchers to explore their use for neoplasms with aberrant CD20 expression. There are some case reports describing CD20+ T-cell lymphomas treated with rituximab, with conflicting results [18-22]. Whereas one report showed a good response of CD20+ T-cell lymphomas to rituximab with gemcitabine, oxaliplatin, and L-asparaginase [18], most reports show that rituximab was not effective or has very limited therapeutic effect. In one case, a patient died of acute tumor lysis syndrome induced by rituximab [19]. Two other patients had relapses at 10 and 16 months, respectively [20]; CD20 expression was lost in the relapsed lymphomas in both cases. In another case, the effect of rituximab was limited, probably because CD20 was only partially expressed on tumor cells [21]. A report in 2015 showed CD20+ primary gastric T-cell lymphoma poorly responded to initial treatment with rituximab plus CHOP (cyclophosphamide, doxorubicin hydrochloride [hydroxy daunomycin], vincristine sulfate, and prednisone) [23].
Theoretically, anti-CD20 agents should have at least a modest effect on neoplasms with aberrant CD20 expression, but reports indicate these agents would not have any significant effect. Huang et al. [1] discussed cases of CD20-positive extranodal NK/T-cell lymphomas with discordant expression of CD20 between the primary and disseminated lesions. This discordant expression is also seen among patients whose diseases relapse and no longer have CD20 expression after receiving anti-CD20 agents [24]. Similar cases have been seen in the literature [4, 6]. As seen in Table 1, of all the reported patients diagnosed with CD20+ NK/T cell neoplasms, none received anti-CD20 targeted therapy [1, 2, 6, 7, 12, 13]. In a leukemia as aggressive as ANKL, the use of an anti-CD20 agent may be moot, but more studies would need to be done to completely rule it out as a helpful therapeutic option.
Despite the aberrant CD20 expression seen in our case, the patient’s clinical course seemed to align with what was expected. In addition, although rituximab was considered, it was not used; therefore, its potential benefit in this case remains unknown. We believe that adequate work-up (IHC stains, flow cytometry, and T- and B-cell gene rearrangement studies) in correlation with the patient’s aggressive clinical history resulted in an accurate diagnosis. Regarding cytogenetics, ANKL is sometimes found to have loss of 7p or 17p and gain of 1q [17, 24]. Cytogenetic analysis ruled out any obvious chromosome abnormalities for this case; however, there may have been an advantage to further genetic testing to search for functional mutations specific to ANKL or to aberrant CD20 expression. We are certain that our case report and the ANKL literature would have benefited from those results.
Conclusion
ANKL is a rare and aggressive disease, making innovations in therapeutics and improvements of patient’s survival difficult. Survival outcomes of ANKL are very poor. It is unclear whether any CD20+ NK/T-cell neoplasm would benefit from rituximab therapy or whether rituximab offers any hope for a cure. Given its rarity, a larger cohort of NK/T-cell neoplasms with aberrant CD20 expression is needed to further investigate this disease as well as the significance of anti-CD20 targeted therapy.
Acknowledgments
Editorial assistance was provided by Daley Drucker and Gerard Hebert of the Moffitt Cancer Center Office of Scientific Publishing; no compensation was given beyond their regular salaries. The authors have no conflicts of interest to declare.
References
- Huang Y, Chen S, Wei R, et al. CD20-positive extranodal NK/T cell lymphoma: clinicopathologic and prognostic features. Virchows Arch. 2020; 477: 873-883.
- Jiang Q, Liu S, Yang Y, et al. CD20-positive NK/T-cell lymphoma with indolent clinical course: report of case and review of literature. Diagn Pathol. 2012; 7: 133-133.
- Miyazaki K, Ohsaka M, Suzuki Y, Danbara M, Horie R, Higashihara M. CD20-positive T-cell large granular lymphocyte leukemia: Case report and review of the literature. Intern Med. 2009; 48: 1443-1447.
- Sohani AR. Falling prey to a wolf in sheep’s clothing: T and NK cell neoplasms with aberrant CD20 expression. Virchows Arch. 2020; 477: 897–899.
- Tamayose K, Sato N, Ando J, Sugimoto K, Oshimi K. CD3-negative, CD20-positive T-cell prolymphocytic leukemia: Case report and review of the literature. Am J Hematol. 2002; 71: 331–335.
- Tsai Y, Chen C, Wu Y. CD20-Positive nodal natural killer/T-cell lymphoma with cutaneous involvement: CD20-Positive NK/T-cell lymphoma. J Cutan Pathol. 2015; 42(9): 639–644
- Zhang Y, Wang K, Tan Q, et al. Primary breast CD20-positive extranodal NK/T cell lymphoma with stomach involvement: a case report and literature review. Diagn Pathol. 2021; 16: 103.
- Ortolani C. Aggressive NK cell leukemia. In: Flow Cytometry of Hematological Malignancies. Second edition. Hoboken, New Jersey: John Wiley and Sons Ltd; 2021. p266.
- Swerdlow S, Campo E, Harris N, et. al. Aggressive NK-cell leukemia. In: WHO Classification of Tumors of Haematopoietic and Lymphoid Tissues. Revised Fourth edition. Lyon, France: International Agency for Research on Cancer; 2017. p353-354.
- Syrykh C, Péricart S, Lamaison C, Escudié F, Brousset P, Laurent, C. Epstein–Barr virus-associated T- and NK-cell lymphoproliferative diseases: A review of clinical and pathological features. Cancers (Basel) 2021; 13: 3315.
- Lima M. Aggressive mature natural killer cell neoplasms: from epidemiology to diagnosis. Orphanet J Rare Dis. 2013; 8: 95.
- Huang YH, Huang CT, Tan SY, Chuang SS. Primary gastric extranodal natural killer/T-cell lymphoma, nasal type, with acquisition of CD20 expression in the subcutaneous relapse: report of a case with literature review. J Clin Pathol. 2015; 68:943-945.
- Gill HS, Lau WH, Chan AC, et al. CD20 expression in natural killer T cell lymphoma. Histopathology. 2010; 57: 157-159.
- Kobold S, Merz H, Tiemann M, et al. Primary NK/T cell lymphoma nasal type of the stomach with skin involvement: a case report. Rare Tumors. 2009;1: e58.
- Ando J, Sugimoto K, Ando M, Isobe Y, Sasaki M, Oshimi K. CD20-positive extranodal NK-cell lymphoma, nasal-type. Eur J Haematol. 2008; 80: 549-550.
- Guan J, Lin W, Liu W, Hui D. Primary central nervous system extranodal NK/T-cell lymphoma, nasal type with CD20 expression: Case report and review of the literature. Neuropathology. 2023.
- Hue SS, Oon ML, Wang S, Tan S, Ng S. Epstein–Barr virus-associated T- and NK-cell lymphoproliferative diseases: an update and diagnostic approach. Pathology 2020; 52: 111–127.
- Shao Y, Bai C, Sun J, Gao X. T-cell lymphoma with abundant CD20 expression showing a good response to rituximab with gemcitabine, oxiplatin, and L-asparaginase (R-pGEMOX): A case report. Medicine (Baltimore). 2018; 97: e0199.
- Hirata Y, Yokote T, Kobayashi K, et al. Rituximab for the treatment of CD20-positive peripheral T-cell lymphoma, unspecified. Leuk Res. 2009; 33: e13-16.
- Mangogna A, Cox MC, Ruco L, Lopez G, Belmonte B, Di Napoli A. Rituximab plus chemotherapy provides no clinical benefit in a peripheral T-cell lymphoma not otherwise specified with aberrant expression of CD20 and CD79a: A case report and review of the literature. Diagnostics (Basel). 2020; 10: 341.
- Kamata M, Sugaya M, Miyagaki T, et al. A case of CD20-positive peripheral T-cell lymphoma treated with rituximab and multiagent chemotherapy. Int J Dermatol. 2014; 53: e24-26.
- Tschetter AJ, Zafar F, Moye MS, et al. CD20+ cutaneous T-cell lymphoma with phenotypic shift after treatment with rituximab: Case report and review of the literature. JAAD Case Rep. 2020; 6: 308-310.
- Kakinoki Y, Hashiguchi J, Ishio T, Chiba K, Niino D, Ohshima K. CD20-positive primary gastric T-cell lymphoma poorly responding to initial treatment with rituximab plus CHOP, and a literature review. Int J Hematol. 2015; 102: 702-708.
- Nazarullah A, Don M, Linhares Y, Alkan S, Huang Q. Aggressive NK-cell leukemia: A rare entity with diagnostic and therapeutic challenge. Human Pathology Case Reports 2016; 4: 32–37.