Case Study
Acute Myeloid Leukemias with Variant RUNX1::RUNX1T1: Report of Three Cases
Xia Li1,2,*, Guang Liu1,3,*
1Department of Pathology, University of Arizona College of Medicine-Phoenix, Phoenix, AZ 85004; 2Shengting Group, Hangzhou, China 311100; 3Genetics/Genomics Division, Sonora Quest Laboratories, Phoenix, AZ 85034.
Abstract
Chromosomal translocation t(8;21) occurs in 5-12% of acute myeloid leukemia (AML) patients. It is one of the best-known recurrent chromosome aberrations in AML that usually correlates with AML with maturation (M2). The translocation results in an in-frame fusion of two genes, generating a chimeric protein composed of one N-terminal domain from the RUNX1 gene and four C-terminal domains from the RUNX1T1 gene. Because the presence of t(8;21) is diagnostic of AML and the prognosis of AML with t(8;21) is usually favorable, detection of t(8;21) has diagnostic, prognostic, and therapeutic implications. Variants of the t(8;21) involving chromosomes 8, 21 and other chromosomes account for approximately 3% of all t(8;21) cases found in AML patients. The clinicopathologic features of AML cases carrying variant t(8;21) are less well-characterized. Conventional cytogenetics and fluorescence in situ hybridization can identify the typical t(8;21) but may miss the variants due to insertion or cryptic translocation, and molecular technologies such as PCR or next-generation sequencing (NGS) is required to detect the abnormalities. Here we report three AML cases with variants of t(8;21) detected using an integrative approach of cytogenetics and molecular genetics analyses. This study illustrates the advantage of using NGS technology in the identification of variant translocations involving RUNX1::RUNX1T1.
Keywords
AML; RUNX1::RUNX1T1; diagnosis; prognosis; cytogenetics; next-generation sequencing
*Correspondence:
Xia Li, Sonora Quest Laboratories, 424 S 56th Street, Phoenix, AZ 85034. Email: Xiasweet@gmail.com. Guang Liu, Sonora Quest Laboratories, 424 S 56th Street, Phoenix, AZ 85034. Guang.liu@sonoraquest.com.
Introduction
Acute myeloid leukemia (AML) with RUNX1::RUNX1T1 is characterized by a fusion of the RUNX1 gene on chromosome 21q22.1 and the RUNX1T1 gene on chromosome 8q22, resulting from the translocation t(8;21)(q22;q22.1). This is one of the core-binding factor leukemias and one of the most common subtypes of AML with recurrent genetic abnormalities that are associated with a favorable outcome [1]. The RUNX1::RUNX1T1 fusion leads to the disruption of the normal function of the core-binding factor and results in leukemogenesis by blocking myeloid maturation and differentiation [2]. Aside from t(8;21), other secondary chromosomal aberrations seen in AML with t(8;21) include deletion of chromosome 9q and loss of an X chromosome in females or loss of a Y chromosome in males [3].
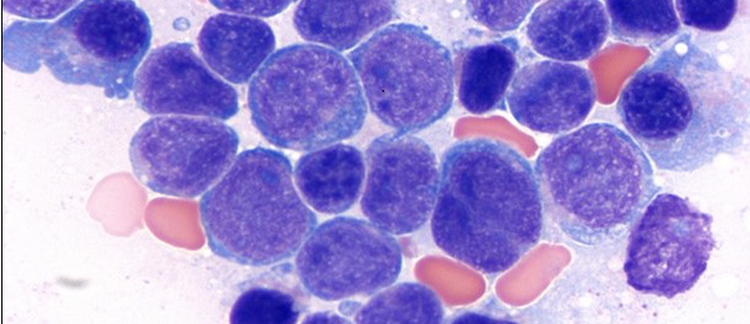
Blasts in this AML category are large with abundant basophilic cytoplasm, often containing numerous azurophilic granules and perinuclear halo (clearing), with fewer monocytes and increased eosinophil [4, 5]. The immunophenotype of this category is characterized by high CD34 expression and aberrant expression of CD19 and cytoplasmic CD79a, with abnormal neutrophil maturation. HLA-DR, CD13, myeloperoxidase, and PAX5 are often expressed, with weak or no expression of CD33. Blasts are usually positive for myeloperoxidase [6-10].
Most patients in this category have higher rates of complete remission and long-term disease-free survival when treated with intensive consolidation therapy (e.g., high dosage of cytarabine) [11, 12]. Several concurrent mutations play a role in modulating the proliferative potential of cells, including mutations in KIT, FLT3, NRAS, KRAS, and possibly JAK2 [1, 13]. The presence of KIT p.D816 in adults correlates with a lower relapse-free survival rate, while hyperdiploidy and/or the presence of del(9q) is associated with longer overall survival [14]. A high (≥2) mutation burden is associated with inferior outcomes [15, 16]. FLT3 mutations have been seen in up to 16% of t(8;21) patients; FLT3-ITD mutations with a high allelic burden are likely to confer inferior survival, while FLT3-TKD is associated with a better outcome [1].
Patients who do not achieve major molecular remission after consolidation therapy are at high risk for relapse and may benefit from allogeneic stem cell transplant therapy [17]. Detection of measurable residual disease either by flow cytometry or PCR-based techniques is associated with lower complete remission rates and shorter survival, even after transplantation [18].
In general, the translocation t(8;21) can be detected as the only genetic abnormality or as part of more complex abnormalities. If t(8;21) is detected in a patient with bone marrow pathology, the diagnosis of AML can be made based on this abnormality alone. Whether the detection of the fusion gene can be used for the evaluation of minimal residual disease and risk of leukemia relapse remains to be clarified [19].
Variants of the t(8;21) involving chromosomes 8, 21 and other chromosomes account for approximately 3% of all t(8;21)(q22;q22) in AML patients. One of the challenges to identifying the variants of the t(8;21) is their likelihood of being missed by conventional cytogenetics and fluorescence in situ hybridization (FISH) analyses. The three cases presented here highlight the importance of the combination of approaches, i.e., standard karyotyping, FISH, PCR, or NGS, for the detection of variants of t(8;21).
Case Report
Case 1
A 68-year-old male presented with a near syncopal episode and was found to have pancytopenia. He also had systemic mastocytosis observed on bone marrow biopsy. He denies any fevers, chills, chest pain, shortness of breath, palpitations, abdominal pain, nausea, vomiting, or diarrhea. He did note chronic, intermittent, moderate to severe, non-radiating, sharp, aching, right shoulder pain.
Flow cytometry analysis detected 46% abnormal myeloblasts expressing dim CD45, partial CD34, dim CD13, CD117, dim HLA-DR, partial CD56 and dim CD19. These findings were consistent with acute myeloid leukemia.
The morphology analysis on peripheral blood smear and bone marrow revealed pancytopenia and 50% circulating blasts from the peripheral blood and hypercellular bone marrow (60%) with systemic mastocytosis and associated hematological neoplasm represented by acute myeloid leukemia (87% blasts) (SM-AHN).
Genetic tests ordered for this patient included karyotyping analysis, FISH for AML panel, RT-PCR for RUNX1::RUNX1T1 rearrangement, FLT3 mutation analysis, and NGS Hematology Molecular Profile of the bone marrow.
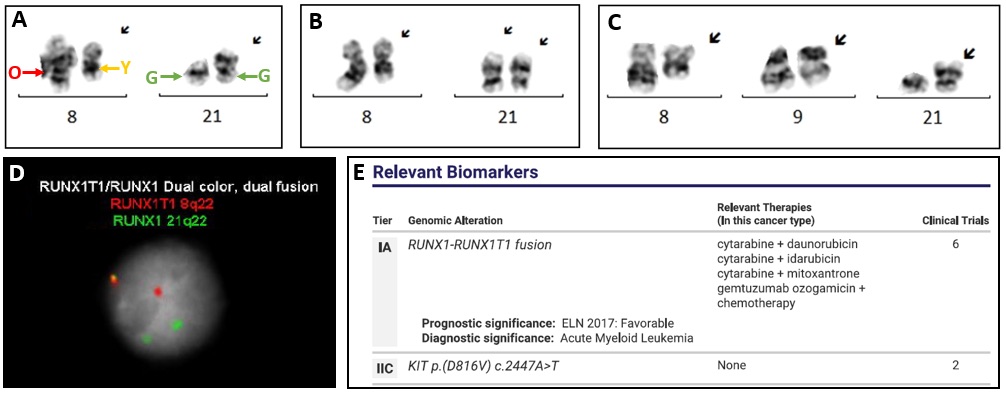
Chromosome analysis revealed a 3-way translocation t(8;21;21)(q22;p13;q22), resulting in the fusion of the RUNX1::RUNX1T1, in 22 of 22 metaphase cells examined (Figure 1A). Fourteen cells showed additional two copies of the derivative chromosome 21 which resulted from t(8;21;21) (Figure 1B). The karyotyping also revealed del(9q) in one of the 20 cells analyzed (Figure 1C).
FISH for AML panel was also performed on interphase nuclei using probes localized to the D5S721 (5p15.2), EGR1 (5q31), D7Z1 (7cen), D7S486 (7q31), D8Z2 (8cen), RUNX1T1 (8q22), ABL1 (9q34.12), KMT2A (11q23), PML (15q24.1), CBFB (16q22.1), RARA (17q21.1), D20S108 (20q12), RUNX1 (21q22.3) and BCR (22q11) regions. Two hundred nuclei were examined, and the results demonstrated an atypical RUNX1::RUNX1T1 rearrangement in 164/200 (82.0%) of the cells scored. There was only 1 red signal indicating a partial deletion of RUNX1T1 (Figure 1D, 1F1R2G). The derivatives of t(8;21;21) were also labeled to show the corresponding signals by FISH (Figure 1A): a fusion signal on der(8), a red signal on the normal chromosome 8, a green signal on the normal chromosome 21, and a green signal on der(21).
Reverse transcription-polymerase chain reaction (RT-PCR) in the reference labs detected the RUNX1::RUNX1T1 fusion transcript with a RUNX1::RUNX1T1 / ABL1 ratio of 10.14139. The FLT3 mutation analysis was negative. An NGS panel that includes 45 targeted genes (DNA) and 35 fusion driver genes (RNA) was conducted in our lab, and the results showed a RUNX1::RUNX1T1 fusion and a KIT p.(D816V) c.2447A>T mutation (Figure 1E).
The results of karyotyping, FISH, RT-PCR, and NGS from this patient were concordant with variant t(8;21) withRUNX1::RUNX1T1 fusion in this AML.
Case 2
The patient is a 53-year-old man with a history of alpha-1 antitrypsin deficiency and was recently diagnosed with thrombocytopenia. Flow cytometry of peripheral blood demonstrated 25% blasts. Flow Cytometry on the bone marrow showed an increased blast population with expression of CD56, CD34, CD33 (dim), CD117, CD13 (dim), HLA-DR, CD19 and CD45 (dim). These results indicated a relapsed AML. The patient underwent induction therapy 7+3 (getting cytarabine continuously for 7 days, along with short infusions of an anthracycline on each of the first 3 days) and tolerated the induction well. He went on to high-dose cytarabine (HiDAC) consolidation, which was complicated by hospitalization for neutropenic fever, as well as some self-limiting transaminitis. Unfortunately, he was found to have disease relapse on surveillance bone marrow biopsy and was admitted for re-induction with FLAG-Ida chemotherapy.
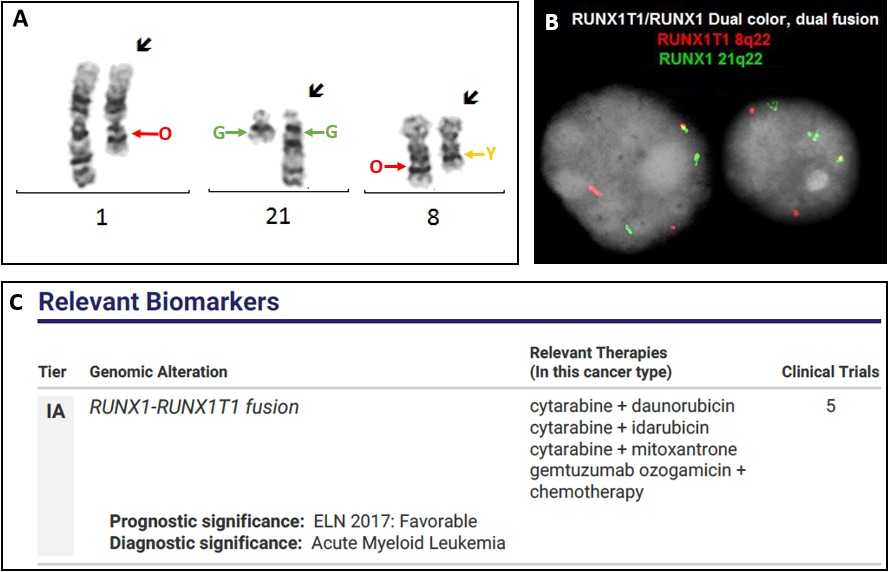
The genetic tests ordered included chromosome analysis, FISH for AML panel, RT-PCR, AML MRD, FLT3 mutation analysis, and NGS Molecular Profile of the bone marrow. Of the 20 cells analyzed, 9 exhibited a loss of the Y chromosome, and a three-way translocation involving 1q, 8q and 21q: [t(1;21;8)(q12;q22;q22)], which is a variant t(8;21) (Figure 2A). The remaining 11 cells were chromosomally normal. FISH for AML panel was performed on interphase nuclei (probe detail as described in case 1). Two hundred nuclei were examined, and the results were positive for a rearrangement involving RUNX1::RUNX1T1 in 74/200 (37.0%) of the cells scored with atypical pattern of 3-way rearrangement involving RUNX1::RUNX1T1 (Figure 2B, 1F2R2G). The derivatives of t(1;21;8) were also labeled to show the corresponding signals by FISH (Figure 2A): a fusion signal on der(8), a red signal on the normal chromosome 8, 1 red signal on der(1), a green signal on the normal chromosome 21, and a green signal on der(21). In house NGS molecular profiling showed RUNX1::RUNX1T1 fusion, concordant with the karyotype and FISH findings (Figure 2C).
Case 3
A 62-year-old female with previous medical history of AML presented with pancytopenia, chest pain and back pain. She denied shortness of breath, dizziness, palpitations, nausea, or vomiting.
Flow cytometric analysis of the bone marrow revealed 23% blasts with a myeloid phenotype, strongly expressing CD13 and CD117. Blasts aberrantly expressed dim CD4 and moderate to strong CD56. This was consistent with a diagnosis of relapsed acute myeloid leukemia.
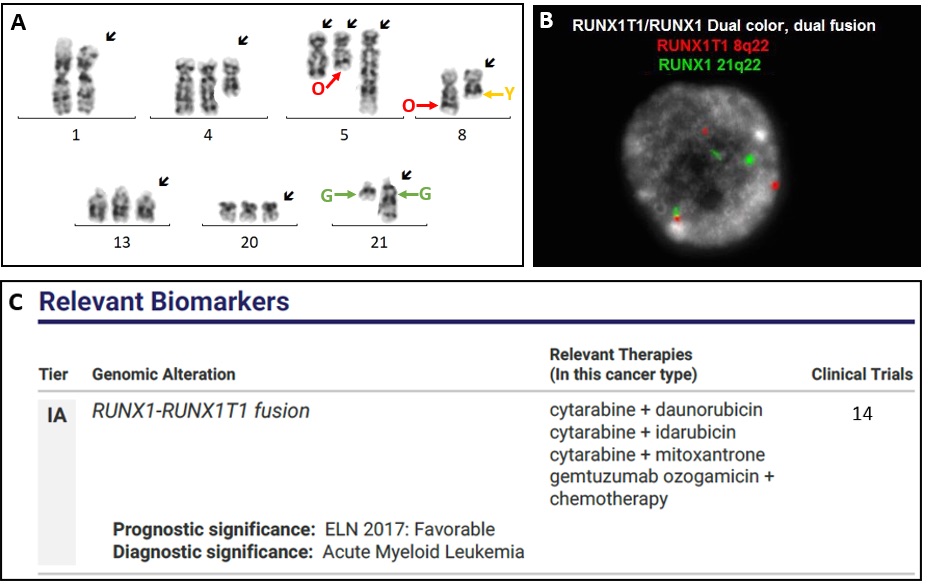
Chromosome analysis was performed initially. Of the 20 metaphase cells analyzed, 9 exhibited a loss of the Y chromosome, and a three-way translocation involving 5q, 8q and 21q, which might be a variant t(8;21) (Figure 3A). The remaining 11 cells were chromosomally normal. FISH for AML panel was performed on interphase nuclei (probe detail as described in case 1), and the results demonstrated multiple abnormalities: Gain of 5p15.2 was observed in 187/200 (93.5%) of cells scored. An atypical RUNX1::RUNX1T1 rearrangement was observed in 190/200 (95.0%) of cells scored (Figure 3B, 1F2R2G). Gain of 20q12 was observed in 190/200 (95.0%) of cells scored. The derivatives of t(5;21;8) were also labeled to show the corresponding signals by FISH (Figure 3A): a fusion signal on der(8), a red signal on the normal chromosome 8, a red signal on der(5), a green signal on the normal chromosome 21, and a green signal on der(21). In-house NGS molecular profiling showed RUNX1::RUNX1T1 fusion, concordant with the results from karyotype and FISH (Figure 3C).
Discussion
AML with t(8;21)(q22;q22) is the typical form presented as part of the group of AML patients with recurrent genetic abnormalities. It is commonly seen in AML-M2, and rarely in M1 or M4 (https://atlasgeneticsoncology.org/haematological/1019/t(8;21)(q22;q22)). This rearrangement has been seen in both children and adults but is more frequently observed in childhood AML, and uncommon in patients over 60 years of age [19-21]. AML with t(8;21)(q22;q22) and inv(16)(p13;q22)/t(16;16)(p13;q22) are both categorized as core binding factor AML, and these cytogenetic abnormalities have a more favorable prognosis when treated with high dose cytarabine [22, 23]. The t(8;21) has been reported in 5 - 12% of de novo AML and results in the fusion protein RUNX1::RUNX1T1 [1, 24-26]. This RUNX1::RUNX1T1 fusion protein regulates the expression of many genes involved in multiple signaling pathways [27]. Complex t(8;21;Var) rearrangement involving a (variable) third chromosome has been described in 3% of AML patients. In terms of prognosis, complete remission (CR) in most cases (90%) can be expected with relatively long disease-free survival when treated with high-dose chemotherapy. Some of the variant translocations with RUNX1::RUNX1T1 fusion transcripts are cytogenetically cryptic and can only be identified with molecular approaches (e.g., quantitative PCR or NGS). In this case report, we present three cases of variant t(8;21) identified in our lab by using karyotyping, FISH, and NGS.
Case 1 was diagnosed as AML by flow cytometry and morphology analysis. Karyotyping showed a variant 3-way translocation involving chromosomes 8, and 21, t(8;21;21)(q22;p13;q22). Two additional clones were also identified by karyotyping: one with an additional derivative chromosome 21, the other clone with del(9q), which is a recurrent chromosome abnormality seen in AML. The clonal evolution seen from chromosome analysis indicates a more aggressive disease process. Both FISH and NGS confirmed the rearrangement of RUNX1::RUNX1T1 although one red signal (RUNX1T1) was lost from der(21). NGS also identified a KIT p.D816V mutation in addition to the RUNX1::RUNX1T1 fusion. KIT mutations occur in 20-30% of cases with RUNX1::RUNX1T1 fusion [28]. The relapse-free survival (RFS) in KIT-mutated patients was inferior to those of unmutated patients. Based on subgroup analysis, KIT mutations had a prognostic impact in patients with RUNX1::RUNX1T1; multivariate Cox regression analysis with stepwise selection revealed that the KIT exon 17 mutation (e.g., D816V) and the presence of extramedullary tumors in patients with RUNX1::RUNX1T1 were poor prognostic factors for relapse-free survival [29]. The patient was treated with decitabine & Venetoclax before he decided to move to his hometown where he would not be able to receive the high-dose chemotherapy.
Case 2 was diagnosed as a relapsed AML by flow cytometry and morphology analysis. Karyotyping revealed a variant 3-way translocation t(1;21;8)(q12;q22;q22) and loss of the Y chromosome, which could be age-related with no clinical consequences. The results from FISH and NGS were concordant with the chromosomal finding. The t(1;21;8) has been reported in several literatures. Kim et al. identified a variant translocation t(1;21;8)(q21;q22;q22) in a 63-year-old female patient with AML. After induction chemotherapy, she had complete remission. There were over 24 such cases in the literature that did not show poorer prognose with t(1;21;8) than those with the classic t(8;21) [30]. Huang et al. reported 4 cases with variant t(8;21), one of them was also t(1;21;8). All 4 patients were treated with combination chemotherapy and are in complete remission [2]. The outcome of the patient was good. He was treated with high dose cytarabine, achieved complete remission, and is now disease-free.
Case 3 was diagnosed as a relapsed AML with a similar approach as for Case 1 and 2. Chromosomal analysis revealed a very complex abnormal karyotype with a 3-way translocation t(5;21;8)(q13;q22;q22), a balanced translocation t(1;5)(p13;q21), gains of add(4p), add(5q), and chromosomes 13 and 20. Literature search did not retrieve any reports with the same 3-way translocation. FISH revealed a typical 3-way translocation signal pattern for RUNX1::RUNX1T1 rearrangement with 1F2R2G. NGS confirmed the rearrangement of this fusion.
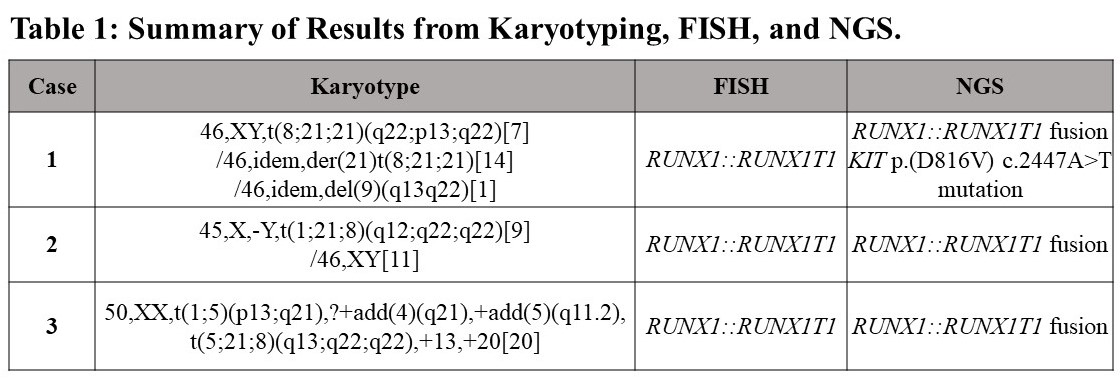
In all 3 cases we presented here, results of karyotyping, FISH and NGS were concordant (Table 1). The patient received induction chemotherapy with HiDAC plus FLAG-IDA. She was not doing well due to chemo-related pancytopenia and intermittently required transfusions of packed red blood cells (PRBCs) and platelets. Patient also had intermittent neutropenic fevers. The patient was deceased after 2 months.
For genetic testing performed in our lab, ideally, the metaphase FISH should be performed to see if the fusion can be identified on the derivative chromosome 8. Due to non-retrievable archived sample, this was not feasible for these 3 cases. Based on the signal patterns by AML FISH, the predicted signal on the karyotype were labeled in Figure 1A, Figure 2A and Figure 3A to help understand the interpretation of the translocation. According to a study by Reikvam et al, there are many variants of t(8;21) reported in the literature. Of the two fusions of RUNX1::RUNX1T1, only the one on derivative chromosome 8 can be detectable by RT-PCR. Other than the simple reciprocal translocation, there are many other mechanisms that can result in fusion such as inversion or insertion involving chromosome 8. These variant rearrangements can be cryptic and easily overlooked by conventional G-banding or FISH [19]. Therefore, NGS should be recommended in case in which discrepant results are seen from karyotype and FISH testing. In the future, chromosome analysis, FISH, or NGS should be ordered to monitor the disease progression and treatment efficacy for the patients.
In conclusion, the t(8;21) variant of AML is a heterogenous subset group of disease with a specific chromosome translocation. The clinical outcome is varied due to limited data, and the prognosis can be modified when complex karyotype and additional DNA mutations are detected. With the advancement of molecular technology (e.g., NGS), more genetic information will be available to aid in a better clinical interpretation, which will contribute to more personalized treatment for patients.
Acknowledgments
The authors declare that they have no conflict of interest.
References
- Al-Harbi S, Aljurf M, Mohty M, Almohareb F, Ahmed SOA. An update on the molecular pathogenesis and potential therapeutic targeting of AML with t(8;21)(q22;q22.1);RUNX1-RUNX1T1. Blood Adv. 2020;4(1):229-238.
- Huang L, Abruzzo LV, Valbuena JR, Medeiros LJ, Lin P. Acute myeloid leukemia associated with variant t(8;21) detected by conventional cytogenetic and molecular studies: a report of four cases and review of the literature. Am J Clin Pathol. 2006;125(2):267-272.
- Han SY, Mrozek K, Voutsinas J, et al. Secondary cytogenetic abnormalities in core-binding factor AML harboring inv(16) vs t(8;21). Blood Adv. 2021;5(10):2481-2489.
- Yabe M, Masukawa A, Kato S, Yabe H, Nakamura N, Matsushita H. Systemic mastocytosis associated with t(8;21) acute myeloid leukemia in a child: detection of the D816A mutation of KIT. Pediatr Blood Cancer. 2012;59(7):1313-1316.
- Johnson RC, Savage NM, Chiang T, et al. Hidden mastocytosis in acute myeloid leukemia with t(8;21)(q22;q22). Am J Clin Pathol. 2013;140(4):525-535.
- Yang DH, Lee JJ, Mun YC, et al. Predictable prognostic factor of CD56 expression in patients with acute myeloid leukemia with t(8:21) after high dose cytarabine or allogeneic hematopoietic stem cell transplantation. Am J Hematol. 2007;82(1):1-5.
- Iriyama N, Hatta Y, Takeuchi J, et al. CD56 expression is an independent prognostic factor for relapse in acute myeloid leukemia with t(8;21). Leuk Res. 2013;37(9):1021-1026.
- Shang L, Chen X, Liu Y, et al. The immunophenotypic characteristics and flow cytometric scoring system of acute myeloid leukemia with t(8;21) (q22;q22); RUNX1-RUNX1T1. Int J Lab Hematol. 2019;41(1):23-31.
- Khoury H, Dalal BI, Nevill TJ, et al. Acute myelogenous leukemia with t(8;21)--identification of a specific immunophenotype. Leuk Lymphoma. 2003;44(10):1713-1718.
- Ray D, Kwon SY, Tagoh H, Heidenreich O, Ptasinska A, Bonifer C. Lineage-inappropriate PAX5 expression in t(8;21) acute myeloid leukemia requires signaling-mediated abrogation of polycomb repression. Blood. 2013;122(5):759-769.
- Hills RK, Castaigne S, Appelbaum FR, et al. Addition of gemtuzumab ozogamicin to induction chemotherapy in adult patients with acute myeloid leukaemia: a meta-analysis of individual patient data from randomised controlled trials. Lancet Oncol. 2014;15(9):986-996.
- Vasu S, Kohlschmidt J, Mrozek K, et al. Ten-year outcome of patients with acute myeloid leukemia not treated with allogeneic transplantation in first complete remission. Blood Adv. 2018;2(13):1645-1650.
- Hollein A, Nadarajah N, Meggendorfer M, et al. Molecular characterization of AML with RUNX1-RUNX1T1 at diagnosis and relapse reveals net loss of co-mutations. Hemasphere. 2019;3(1):e178.
- Ustun C, Morgan E, Moodie EEM, et al. Core-binding factor acute myeloid leukemia with t(8;21): Risk factors and a novel scoring system (I-CBFit). Cancer Med. 2018;7(9):4447-4455.
- Krauth MT, Eder C, Alpermann T, et al. High number of additional genetic lesions in acute myeloid leukemia with t(8;21)/RUNX1-RUNX1T1: frequency and impact on clinical outcome. Leukemia. 2014;28(7):1449-1458.
- Hamosh M. Does infant nutrition affect adiposity and cholesterol levels in the adult? J Pediatr Gastroenterol Nutr. 1988;7(1):10-16.
- Wang Y, Wu DP, Liu QF, et al. In adults with t(8;21)AML, posttransplant RUNX1/RUNX1T1-based MRD monitoring, rather than c-KIT mutations, allows further risk stratification. Blood. 2014;124(12):1880-1886.
- Yalniz FF, Patel KP, Bashir Q, et al. Significance of minimal residual disease monitoring by real-time quantitative polymerase chain reaction in core binding factor acute myeloid leukemia for transplantation outcomes. Cancer. 2020;126(10):2183-2192.
- Reikvam H, Hatfield KJ, Kittang AO, Hovland R, Bruserud O. Acute myeloid leukemia with the t(8;21) translocation: clinical consequences and biological implications. J Biomed Biotechnol. 2011;2011:104631.
- Mrozek K, Marcucci G, Paschka P, Bloomfield CD. Advances in molecular genetics and treatment of core-binding factor acute myeloid leukemia. Curr Opin Oncol. 2008;20(6):711-718.
- Bruserud O, Hovland R, Wergeland L, Huang TS, Gjertsen BT. Flt3-mediated signaling in human acute myelogenous leukemia (AML) blasts: a functional characterization of Flt3-ligand effects in AML cell populations with and without genetic Flt3 abnormalities. Haematologica. 2003;88(4):416-428.
- Byrd JC, Mrozek K, Dodge RK, et al. Pretreatment cytogenetic abnormalities are predictive of induction success, cumulative incidence of relapse, and overall survival in adult patients with de novo acute myeloid leukemia: results from Cancer and Leukemia Group B (CALGB 8461). Blood. 2002;100(13):4325-4336.
- Prebet T, Boissel N, Reutenauer S, et al. Acute myeloid leukemia with translocation (8;21) or inversion (16) in elderly patients treated with conventional chemotherapy: a collaborative study of the French CBF-AML intergroup. J Clin Oncol. 2009;27(28):4747-4753.
- Arber DA, Stein AS, Carter NH, Ikle D, Forman SJ, Slovak ML. Prognostic impact of acute myeloid leukemia classification. Importance of detection of recurring cytogenetic abnormalities and multilineage dysplasia on survival. Am J Clin Pathol. 2003;119(5):672-680.
- Bae SY, Kim JS, Ryeu BJ, et al. Acute myeloid leukemia (AML-M2) associated with variant t(8;21): report of three cases. Cancer Genet Cytogenet. 2010;199(1):31-7.
- Grimwade D, Walker H, Oliver F, et al. The importance of diagnostic cytogenetics on outcome in AML: analysis of 1,612 patients entered into the MRC AML 10 trial. The Medical Research Council Adult and Children's Leukaemia Working Parties. Blood. 1998;92(7):2322-2333.
- Wilde L, Cooper J, Wang ZX, Liu J. Clinical, Cytogenetic, and Molecular Findings in Two Cases of Variant t(8;21) Acute Myeloid Leukemia (AML). Front Oncol. 2019;9:1016.
- Paschka P, Marcucci G, Ruppert AS, et al. Adverse prognostic significance of KIT mutations in adult acute myeloid leukemia with inv(16) and t(8;21): a Cancer and Leukemia Group B Study. J Clin Oncol. 2006;24(24):3904-3911.
- Ishikawa Y, Kawashima N, Atsuta Y, et al. Prospective evaluation of prognostic impact of KIT mutations on acute myeloid leukemia with RUNX1-RUNX1T1 and CBFB-MYH11. Blood Adv. 2020;4(1):66-75.
- Kim H, Moon HW, Hur M, Yun YM, Lee MH. Acute myeloid leukemia with a RUNX1-RUNX1T1 t(1;21;8)(q21;q22;q22) novel variant: a case report and review of the literature. Acta Haematol. 2011;125(4):237-241.