Case Study
Intravascular Large B-Cell Lymphoma Arising in a Spinal Hemangioma
Momin Ahmed1, K. David Li2,*
1Mayo Clinic College of Health Sciences, University of Florida, Gainesville, FL 32611; 2Hematopathology, Department of Laboratory Medicine and Pathology, Mayo Clinic, Jacksonville, FL 32224
Abstract
Intravascular large B-cell lymphoma is a rare subtype of diffuse large B-cell lymphoma characterized by neoplastic growth within the lumen of blood vessels. The disease is difficult to diagnose since the clinical symptoms presentations vary from asymptomatic to central nervous system manifestations and it carries a poor prognosis. Definitive diagnosis often requires multiple biopsies from various areas of the body. We present a case of intravascular large B-cell lymphoma involving capillary hemangioma localized to the spinal column in a 72-year-old male.
Keywords
Intravascular large B-cell lymphoma; diffuse large B-cell lymphoma; hemangioma
*Correspondence:
K. David Li, MD, 4500 San Pablo Road S, Jacksonville, Florida 32224. Phone: (904) 956-3318; Email: Li.Ke@mayo.edu.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is a lymphoid neoplasm characterized by abnormal growths of medium to large B cells. Although typically involving lymph nodes, tumors can form in extranodal locations and in various organ systems. It is estimated that up to 40% of DLBCL presents in extranodal sites [1]. Depending on the stage of the disease, DLBCL has been known to respond well to a regimen of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) [2, 3]. This may be followed by radiation therapy or stem cell transplant depending on the severity of the disease [2, 3]. Intravascular large B-cell lymphoma (IVLBCL) is a rare subtype of DLBCL characterized by the growth of large, atypical B lymphocytes within the lumen of blood vessels [4]. The age-adjusted incidence rate of IVLBCL in the United States is estimated to be approximately 0.1 cases/million. It commonly presents in three different ways, known historically as the Western, Asian, and cutaneous variants [5]. The Western variant is characterized by neoplastic growth in the skin or central nervous system (CNS), whereas the Asian variant often presents with fever, thrombocytopenia, and bone marrow involvement [6]. The cutaneous variant is the least aggressive of the three variants, typically presenting as skin lesions with little to no systemic involvement [5]. Like DLBCL, IVLBCL is typically treated with R-CHOP and radiation, though the prognosis is not nearly as satisfactory. It is estimated that IVLBCL patients retain a 3-year overall survival rate of 11.5% compared to a much larger higher 70% overall survival rate of DLBCL patients in the rituximab treatment era [7, 8]. Given the aggressive nature of the disease, it is critical to understand the multifarious ways in which it presents in order to intervene at an earlier stage. Here we describe an interesting case of IVLBCL arising in a capillary hemangioma within the spinal column.
Case Report
A 72-year-old male presented with worsening bilateral extremity and lower back weakness. Patient reported extreme lower body weakness to the point where he was unable to walk and wheelchair dependent. Notable past medical history included hypertension and hyperlipidemia. There was no reported history of blunt force trauma and no reported history or evidence of underlying immune deficiency. Physical examination did not reveal lymphadenopathy or skin rash/lesions. Laboratory testing at presentation included mild anemia and a normal white blood cell count and differential. LDH was within normal range at 127 U/L (reference range: 122-220 U/L). Infectious work-up including HIV, HSV, Hepatitis B/C, and bacterial and fungal cultures was negative. After initial evaluation by neurosurgery, the patient underwent a L2-S1 fusion, which resulted in very little improvement.
With worsening weakness, an MRI of the entire spine was performed and showed a 5.4 cm epidural mass causing dorsal compression of the thoracic spinal cord from T6-T8 (Figure 1). Additional MRI of the brain and CT of the chest were also performed and showed no evidence of intracranial lesions, adenopathy, or metastatic disease. A thoracic laminectomy and resection of the epidural mass was performed.

Results
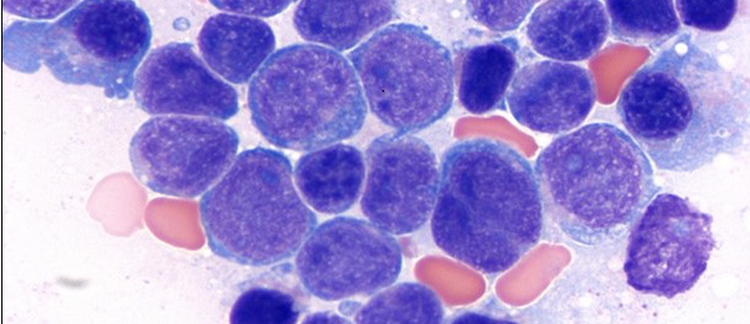
Resection of the T7 epidural spinal mass demonstrated prominent vascular proliferation with an atypical large cell infiltrate exclusively within the lumens of small and intermediate sized vessels (Figure 2). The large cells have irregular nuclei, vesicular chromatin, occasional prominent nucleoli, and moderate cytoplasm. The large cells express CD5, CD19, CD20, BCL2, BCL6, MUM1, and c-MYC. CD10 shows weak partial positivity and MIB-1 is >95% positive. CD138, kappa, lambda, EBV(EBER), and cyclin D1 are negative in the tumor cells. FISH for MYC rearrangement and MYD88L265P mutation analysis were negative. No additional cytogenetic or molecular testing was performed. Based on these findings, a diagnosis of IVLBCL involving capillary hemangioma was made. Bone marrow biopsy was not performed. Additional MRIs of the brain conducted four days after laminectomy showed no intracranial mass or pathologic enhancement.

Follow Up
The patient was started on therapy with rituximab, followed by a high dose of methotrexate, and then two cycles of R-CHOP. Chemotherapy was stopped due to a MRSA PICC line infection and bacteremia. The patient recovered well with a prolonged course of vancomycin. Due to a 6-month interruption in treatment, the patient was deemed unsuitable for continued chemotherapy. To date, the patient’s lymphoma is being treated with a combination of Bruton tyrosine kinase (BTK) inhibitor (ibrutinib), and rituximab infusions. MRI of the spine nine months after the initial diagnosis showed no signs of lymphoma mass recurrence. The patient was discharged back home to follow up with primary oncologist.
Discussion
We describe a case of IVLBCL involving a capillary hemangioma which presented as an epidural spinal mass. Despite the aggressive nature of the disease, our patient was disease free nine months post therapy. To date, only a handful of cases of IVLBCL involving a hemangioma have been reported (Table 1). Hemangiomas are well known to be benign vascular tumors that arise in around 7% of adolescents and 75% of adults >75 years [9,10]. Like in the previously published literature, our patient’s age was consistent with the average age of most IVLBCL diagnoses [11]. Our case is unique in the presentation, presenting as growth within the spinal column rather than a subcutaneous lesion. In fact, the skin exam for this patient was unremarkable. Hirano et al [12] reported a similar case involving the CNS and with little noticeable skin involvement. In that case, a patient presented with right circumorbital pain found to be caused by a mass in the brain. Surgical resection of the mass demonstrated a cavernous hemangioma containing neoplastic B cells. Immunohistochemical analysis of the large lymphocytes was positive for CD20 and CD45, but negative for CD3, CD4, CD5, CD8, and CD30. Interestingly, our case shows CD5 expression. Prior literature has attempted to link CD5 expression to intravascular involvement, estimating that around 38% of IVLBCL cases express CD5 [13,14]. However, given the variable nature of this finding and rarity of the entity, this has yet to be further explored.

Over the past two decades, multiple studies have advocated for the biopsy of various skin lesions and hemangiomas for possible lymphomas, yet very few proved how and why IVLBCL appear to be drawn to hemangiomas [13,15]. Nixon et al [14] attempted to explain this, citing that lymphocytes of IVLBCL are incapable of transvascular migration due to the lack of CD29 and CD54 adhesion molecules. Satoh et al [16] also attempted to explain this relationship, stating that the lymphoma cells may get “trapped” by the vessel-rich structure of hemangioma, unable to proliferate elsewhere. Another explanation may be that hemangioma provides a place for neoplastic lymphocytes to remain undetected before proliferating throughout the body. In any case, this is still ambiguous and requires further investigation.
As far as whether treatments would change if IVLBCL was not localized to a hemangioma also remains unclear. Given the poor prognosis of this disease in general, treatments would likely remain the same (R-CHOP) to ensure no further metastasis of the disease. Based on our case and those reported in the literature, one might propose a subset of IVLBCL that are indolent in clinical behavior and carry a better prognosis; however, this is largely speculative. It is also possible that location, in this case hemangioma, may serve a protective function. At this time, this proves to be a likely hypothesis; however, further research is required to prove this theory. Although we were not able to perform more comprehensive genomic testing on this case other than MYD88L265P, recent genomic studies [20] confirmed the mutational landscape of IVLBCL which included mutations in PIM1, MYD88L265P, and CD79B, as a part of the B-cell receptor/NF-kB pathway, suggesting possible targets for novel therapy.
Conclusion
We present a unique case of IVLBCL arising in a capillary hemangioma. Given its overall poor prognosis, it is imperative to identify the disease at an early stage. While it is uncertain why some IVLBCL form within hemangioma, it may be a positive prognostic factor for these patients.
Acknowledgments
The authors declare that they have no conflict of interest.
References
- Rosai J, Ackerman L. Rosai and Ackerman's Surgical Pathology (9th Edition). St. Louis, MO: Elsevier Mosby 2004. 3080 p.
- Padala SA, Kallam A. Diffuse large B cell lymphoma. In: StatPearls. [Internet].: Treasure Island (FL): StatPearls Publishing; 2022 Jan. 2022 April 28.
- American Cancer Society [Internet]. Treating B-cell non-Hodgkin lymphoma. December 13th, 2022 - [cited December 22 2022]; American Cancer Society, Inc. Available from: http://cancer.org/
- Ponzoni M, Campo E, Nakamura S. Intravascular large B-cell lymphoma: a chameleon with multiple faces and many masks. Blood 2018; 132(15): 1561-1567.
- Boas PV, Cerroni L, Requena L. Intravascular cutaneous disorders. A clinicopathologic review. Am J Dermatopathol 2021; 43(2): 119-136.
- Ponzoni M, Ferreri AJ, Campo E, et al. Definition, diagnosis, and management of intravascular large B-cell lymphoma: proposals and perspectives from an international consensus meeting. J Clin Oncol 2007; 25(21): 3168-3173.
- Adiyaman SC, Alacacioglu I, Danyeli AE, et al. Prognostic factors in elderly patients with diffuse large B-cell lymphoma and their treatment results. Turk J Haematol 2019; 36(2): 81-87.
- Liu Z, Zhang Y, Zhu Y, Zhang W. Prognosis of intravascular large B cell lymphoma (IVLBCL): Analysis of 182 patients from global case series. Cancer Manag Res 2020; 12: 10531-10540.
- The Royal Children's Hospital Dermatology, Plastic Surgery, General Surgery and General Medicine Departments [Internet]. Haemangiomas of infancy (strawberry naevus). In: Kids Health Info. Melbourne, AU. August 16 2018 - [cited December 22 2022]; The Royal Children's Hospital Melbourne. Available from: https://rch.org.au/
- Qadeer HA, Singal A, Patel BC. Cherry Hemangioma. In: StatPearls [Internet]: Treasure Island (FL): StatPearls Publishing; 2022 Jan. 2022 October 3.
- Roy AM, Pandey Y, Middleton D, Broadfoot B, Sasapu A, Veeraputhiran M. Intravascular large B-cell lymphoma: A diagnostic dilemma. Cureus 2021; 13(7): e16459.
- Hirano H, Tashiro Y, Fujio S, Goto M, Arita K. Diffuse large B-cell lymphoma within cavernous hemangioma of the cavernous sinus. Brain Tumor Pathol 2011; 28(4): 353-358.
- Adachi Y, Kosami K, Mizuta N, et al. Benefits of skin biopsy of senile hemangioma in intravascular large B-cell lymphoma: A case report and review of the literature. Oncol Lett 2014; 7(6): 2003-2006.
- Nixon BK, Kussick SJ, Carlon MJ, Rubin BP. Intravascular large B-cell lymphoma involving hemangiomas: an unusual presentation of a rare neoplasm. Mod Pathol 2005; 18(8): 1121-1126.
- Ishida M, Hotta M, Hodohara K, Okabe H. A case of intravascular large B-cell lymphoma colonizing in senile hemangioma. J Cutan Pathol 2011; 38(2): 251-253.
- Satoh S, Yamazaki M, Yahikozawa H, et al. Intravascular large B cell lymphoma diagnosed by senile angioma biopsy. Intern Med 2003; 42(1): 117-120.
- Sakurai T, Wakida K, Takahashi T, Ishida K, Iwata H, Nishida H. Usefulness of senile hemangioma biopsy for diagnosis of intravascular large B-cell lymphoma: A report of two cases and a literature review. J Neurol Sci 2017; 373: 52-54.
- Krokowski M, Sellmann L, Feller AC. Intravascular large B-cell lymphoma within a subcutaneous cavernous haemangioma. Br J Haematol 2010; 151(1): 2.
- Rubin MA, Cossman J, Freter CE, Azumi N. Intravascular large cell lymphoma coexisting within hemangiomas of the skin. Am J Surg Pathol 1997; 21(7): 860-864.
- Gonzalez-Farre B, Ramis-Zaldivar JE, Castrejón de Anta N, et al. Intravascular large B-cell lymphoma genomic profile is characterized by alterations in genes regulating NF-?B and immune checkpoints. Am J Surg Pathol 2023; 47(2): 202-211.
